Is this site about hysterectomy?
Largely, no. It's about the consequences of hysterectomy as it relates to effects on ovaries, and the research touches on hysterectomy from time to time, but the main focus is on the detrimental effects of ovarian failure or removal.
Though hysterectomy and ovary removal are commonly misunderstood, removing the ovaries is not part of a hysterectomy. A hysterectomy only involves the uterus. If the ovaries are removed, that is a separate procedure called an oophorectomy, pronounced OH-uh-forectomy.
Why is ovary removal a problem?
For two reasons not well-understood by the public. It is not taught outside of medicine, for whatever reason, the public does not realize that:
1) the ovaries are a crucial, lifelong part of the endocrine system, and
2) the ovaries keep producing hormones a woman needs for a woman's entire life - this doesn't end at menopause - only egg production ends
This lack of understanding has allowed this surgery to continue at the rate it has for decades.
Both patients and legislators must come to understand what doctors already know: there are serious health risks involved in ovary removal, even for women past the age of menopause, that make the surgery terribly harmful and of no benefit to women outside of the 2% of women with increased breast or ovarian cancer risk.
This site contains data from hundreds of UCLA, Mayo Clinic, Harvard, NIH - you name it - studies about the increased risk of removing this part of the endocrine system, including: premature death, Parkinson’s, Alzheimer’s, dementia, cognitive impairment, memory impairment, osteoporosis/fracture, cardiovascular disease, stroke, arteriosclerosis, sexual dysfunction, lung cancer, type II diabetes and metabolic disorder, depression, and glaucoma. (see Citations)
If a woman has lost her ovaries, harm has already been done.
What are the serious health consequences?
What is this slide about and why does it matter?
Endocrine dyscrasia: "an age-related dysregulation of the hypothalamic-pituitary-gonadal (HPG) axis and is associated with dyotic signaling and the induction of neurodegenerative cascades within the brain."
Translation: The rate at which our bodies' health declines is directly tied to the connection between the ovaries (or testes) and the brain (hypothalamus & pituitary). The neurodegenerative diseases described can include ALS, Parkinson's, Alzheimer's, and Huntington's, which occur as a result of neurodegenerative processes. 287, 343 They are only a few of the risks introduced when this part of our bodies is disrupted.
HPG axis: hypothalamic-pituitary-gonadal axis. Sounds complicated but...
Translation: The connection between the brain and the ovaries (or testes). "g" is for "gonad": ovaries and testes are the gonads. This slide is saying that if that axis is messed up it results in a global and pervasive deterioration of bodily function and leads to premature aging. Put more simply, when gonads malfunction, people get sick and age more quickly. It is a signal to the body that the person is older.
That's with malfunctioning or aging ovaries. So what happens when the ovaries are gone entirely?
Without their ovaries, study after study has demonstrated that women get sick from a range of serious diseases such as premature death, Parkinson’s, Alzheimer’s, dementia, cognitive impairment, memory impairment, osteoporosis/fracture, cardiovascular disease, stroke, arteriosclerosis, sexual dysfunction, lung cancer, type II diabetes and metabolic disorder, depression, and glaucoma, as proven through decades of studies at the Mayo Clinic, UCLA. It is a very serious issue. 1-20, etc
The diseases that result are described in detail in the letter on the home page, and in the Citations section. Because this happens to women for no reason every day, this is not just a medical fact: it's a terrible truth.
Using informed consent forms to excuse anything:
When other surgeons learn that this is being done to healthy women at no risk, they cannot believe that OB/GYNs are performing this surgery. It represents nothing other than making healthy women ill. If you are familiar with the OB/GYN specialty's attitude toward use of a morcellation device when treating fibroids, this may not surprise you. OB/GYN surgeons believed that 1 in 1,000 fibroids was sarcoma (a form of cancer).
The truth was that they were using the wrong denominator to figure out the rate of cancer, so when the FDA was finally called upon to investigate, they learned that the truth was that in 1 in 352 cases where women have surgery to treat fibroids, the fibroids were actually sarcoma. In either case, OB/GYN surgeons were still going ahead and chopping up what they believed had a chance of 1 in 1,000 of being cancer at least 60,000 times a year. Worse, they were doing this during elective (meaning optional, not life-threatening) surgeries where they could simply have performed the surgeries as they always had before morcellators came along - either with a larger incision that would allow the uterus and fibroids to be removed whole, or vaginally, which would also allow the uterus and fibroids to be removed intact. Instead, cancer was sprayed throughout patients' systems, making it infinitely more difficult, if not impossible, to cure. Patients died, but the ACOG's reaction was to study the results rather than to stop that method of performing the surgery.
As with ovary removal, these physicians think making patients sick so long as they've signed a surgical consent form is ok. The ACOG wrote this a full year after they were forced to confront what they had been doing to patients: "it is important for each patient and her doctor to communicate fully about the risks and benefits of all procedures, including surgical options, so that she is able to make an informed and voluntary decision about the care that she receives." They said they were reviewing data. As with the removal of healthy ovaries, there is absolutely no need to review data. There is an urgent need to stop. The ACOG is "currently undertaking a thorough and deliberate review of the published scientific literature about power morcellation and malignancy in gynecologic surgery."
http://www.acog.org/About-ACOG/Announcements/FDA-Issues-Safety-Communication-on-Laparoscopic-Uterine-Power-Morcellation
This "it's all up to the patient" attitude was the same we encountered when reaching out to the president of the ACOG at the beginning of June. When asked about the practice and the harm done, he did not deny it. He simply said that it was up to the patient.
It is not wrong to question the judgment of a practice area that thinks that this risk is permissible. Imagine thinking that there is any circumstance under which it is ok to do this. These physicians are totally resistant to the idea that some questions should simply not be asked. For this reason, we have to speak about this in very simple terms. Options that harm patients and offer either no benefit or a benefit that is not outweighed by risk should not be offered. When a surgeon offers a harmful option to a patient, that is malfeasance. The surgeon may claim that the patient agreed to the surgery, but the surgeon intuitively knows what is written in the ACOG's own Code of Ethics - that if a surgeon offers a procedure to a patient, that patient will assume it is safe and beneficial. A bias is introduced just through the act of offering it. Patients need to be able to trust their doctors.
In the case of the ovaries, they've known for at least a century that the ovaries have a lifelong function, but they remove them for no reason in the hundreds of thousands a year. It's hard to imagine another medical specialty doing this.
Why would surgeons do this?
Hopefully a Congressional hearing will get to the bottom of this question. This surgery is only beneficial for surgeons' and pharma's wallets. Over the past several decades, the surgeons ignored what they knew about their patients' bodies. and took a $40B situation and made it a $500B situation through a $30K surgery and subsequent need for hormone therapy, at the expense of their patients' health.
Congress may not want to take this issue on. It's going to be big and it's going to be a headache. The public must demand that they address this. It is one of the most important aspects of their job. For that reason, a letter detailing our concerns and the urgency of the issue has been sent to members of the Senate Committee on Health:
Sen. Patty Murray
Sen. Lamar Alexander
Sen. Al Franken
Sen. Elizabeth Warren
Sen. Bernie Sanders
It's also been sent to our local Virginia congresspeople:
Sen. Mark Warner
Sen. Tim Kaine
House Rep. Gerry Connolly
We included President Obama and Vice President Biden in our letter, and mailed hard copies and sent emails to each of them.
Sen. Alexander wrote back about Planned Parenthood, so we wrote back correcting the issue being presented.
Sen. Warner sent a short form letter back, saying thanks for the telling me your thoughts. The Washington Post reports that he was busy that week meeting with folks from Etsy.
The only congressperson who has responded so far is Congressman Gerry Connolly, whose Legislative Director, Dominic Bonaiuto, has said he will talk to us again next week (week of Aug. 2, 2015).
Other groups whom we believe should be playing a role but who have not, to-date:
The ACLU - Susan Herman
DOJ, Civil Rights Division - Vanita Gupta
National Women's Law Center - Gretchen Borchelt
Equal Means Equal/ERA Coalition - Jessica Neuwirth, Bettina Hager
Attorney Gloria Allred
NPR - Graham Smith, Audie Cornish
Washnigton Post - Amy Goldstein, Lena Sun
Wall Street Journal - Jennifer Levitz
New York Times
Chicago Tribune - Wes Venteicher
Boston Globe - Lazar, Kowalczyk
LA Times
Human Rights Watch
The Carter Center
Public Justice
Institute for Women's Policy Research - Hartmann, Gault
National Women's Health Network
- Cindy Pearson
What is the goal of this site?
The goal is to help people understand the harm done when the ovaries are removed in women who are not at proven increased risk of breast or ovarian cancer, and to encourage women (and men!) to write or call their legislators to demand Congressional hearing into why this practice has been permitted to persist, and to call for a moratorium on this practice in women who are not at proven increased risk.
http://www.house.gov/representatives/find/
How often are healthy ovaries removed?
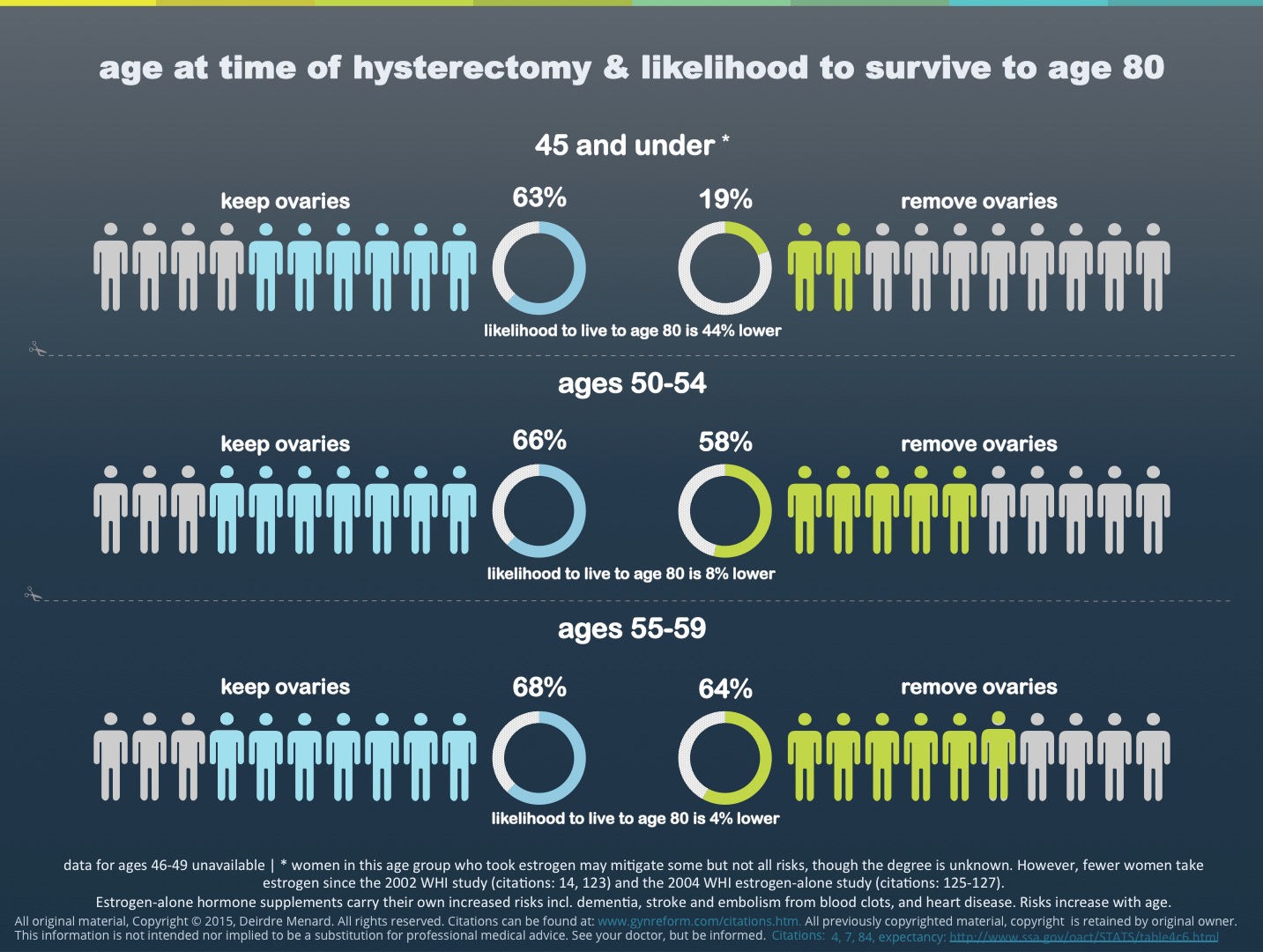
365,000 times per year in the U.S. Removing healthy ovaries is done in 55% of 665,000 hysterectomies a year, even though the procedures are unrelated. The surgeons are just in the neighborhood. At least another 45,000 women lose the function of their ovaries after a hysterectomy due to low blood supply, resulting in a total of 410,000 women a year who will die prematurely as a result of this surgery. 1-20, 37
This has happened to women in the millions already and, each day that goes by, it happens to 1,000 more. #1000womenaday
What about BRCA 1 and 2? Women at high risk?
Only 2% of all U.S. women are at increased genetic risk of either breast or ovarian cancer, and ovarian cancer risk is only reduced by 85%, not entirely prevented, when the ovaries of a high-risk woman are removed. 101, 272
Why only 85%? Cancer cells migrate to other body parts before the ovaries (or, to be consistent with more recent thinking, the fallopian tubes) are removed.
In addition, since about 2010, studies increasingly point to the idea that epithelial cancer that was thought to start in the ovaries likely actually originates in the fallopian tubes, which would mean that the risk could be reduced without doing harm to endocrine organs. 260, 261, 264 Women with a predisposition to these cancers, should see a genetic counselor. In all other women, the surgery offers no benefit, only risk.
For women not determined by genetic testing to be at high risk, their ovarian cancer risk is only reduced through this very harmful surgery by about 1/2 of 1%. 84
What has happened to the ovarian cancer mortality rate since the practice of removing healthy ovaries became so common?
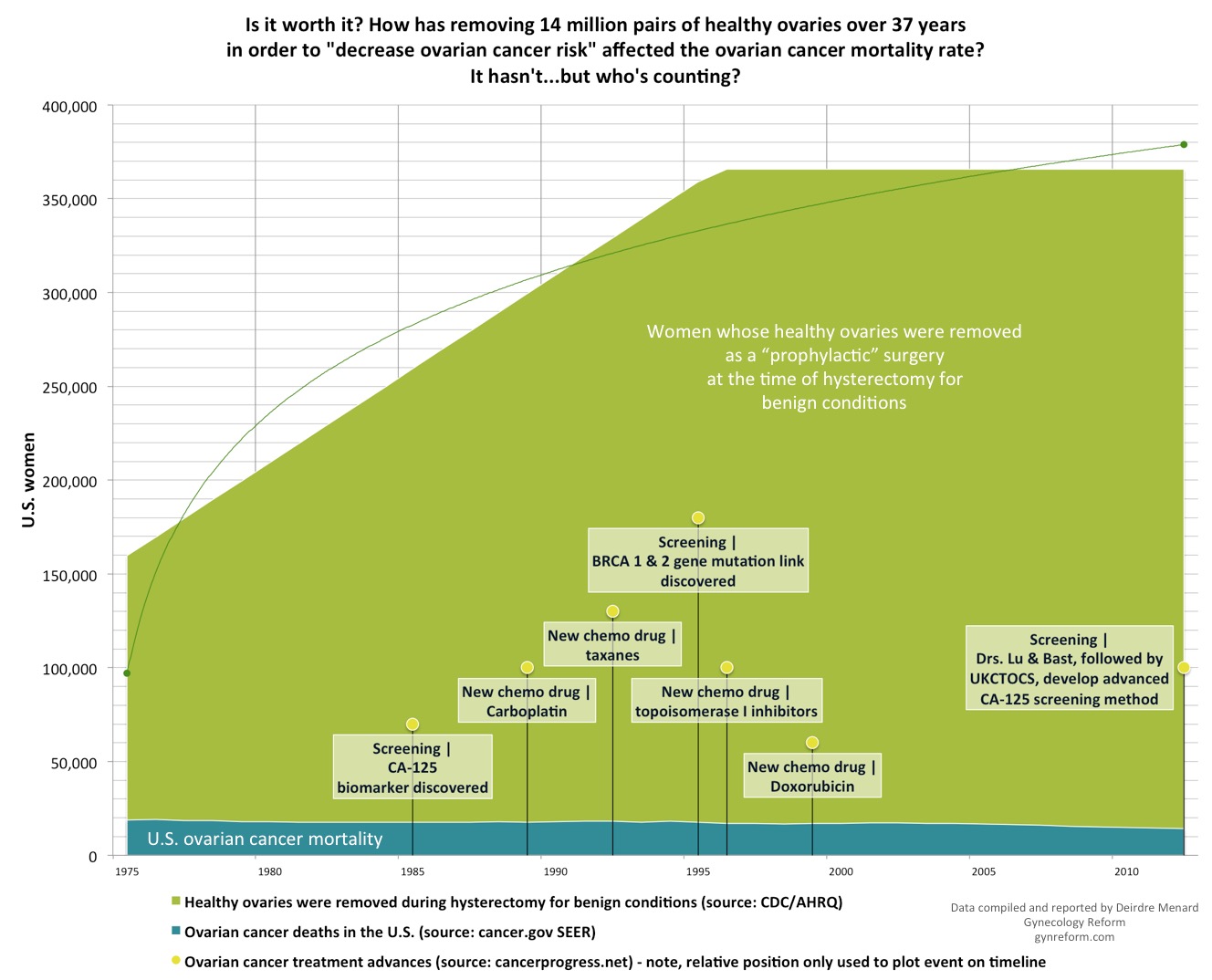
Despite the fact that 365,000 healthy sets of ovaries have been removed each year at hysterectomy for decades, and with all of the recent advances in medication and chemotherapy, the ovarian cancer mortality rate has stayed where it was before this became a common practice. About 14,200 women die of ovarian cancer per year. 221 This surgery is offering zero benefit.
Don't ovaries stop working after menopause, anyway?
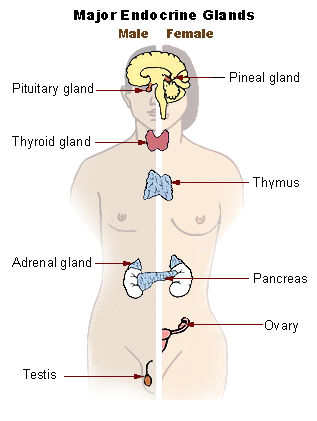
No. Though the ovaries are often referred to as part of the reproductive system, and obviously do play a role there, it's more accurate to say that they are endocrine organs. They should be left in place where they continue to live on, producing hormones, as a vital part of the endocrine system for a woman's entire life. 28, 29 , 49, 116 , 118
Like the hypothalamus, thyroid, thymus, islets of Langerhans in the pancreas, or adrenal glands, this is what the ovaries are - a very basic, necessary part of this system. This system regulates resistance to disease, healthy metabolism, and regulation of things like blood pressure, sleep, appetite, artery integrity, etc etc.
There is a changeover in the way ovaries function at menopause, which is why women have issues at that time with hot flashes, but once the changeover takes place, the ovaries start back up in their new role. They are not disposable; they are still very much needed. Removing healthy ovaries is no less desctructive than removing the thyroid, the pancreas, or any other part of the endocrine system. 111, 287
But I trust my doctor. If she/he says I should remove them to prevent cancer, shouldn't I trust her/him?
If you have had genetic counseling and you have been determined to be at high risk, that is a different decision from removing them if you are among the 98% of women who are not at risk.
It is important to understand that the ACOG, the member organization that 57,000 OB/GYNs belong to, has put out patient brochures that say that the ovaries stop functioning at menopause despite the fact that gynecological studies dating back to at least 1912 state that they knew, even at that time, that that is untrue. That, and the 55% removal rate, compared to, say a 20% removal rate in the UK, should at least concern you and make you consider a second or third opinion. 228, 308
Can't I just replace what is missing with estrogen?
No. Without ovaries, millions of women have paid big pharma about $6,000 for medication they would otherwise not have needed for, on average, 5 years. That hormone medication only provides estradiol, and comes with its own risks. Post-menopausal ovaries are tied to the production of the hormones DHEA, estradiol, estrone, androstenedione, and testosterone, as well as activin and inhibin. Without them, other parts of the endocrine system try to pick up the slack, but cannot.
Is your work in any way related to the HERS Foundation?
No.
I have been asked this question a few times since my work began, so I feel the need to address it here.
The HERS Foundation and I differ on some of the issues. It's important not to conflate castration with removal of other parts of the body. Only removal of the ovaries can be referred to accurately as castration. 80
As a result, this subset of affected women believes that the removal of the uterus has been as detrimental to their wellbeing as the removal of the ovaries, despite the fact that the overwhelming body of evidence says that the health impacts of the two procedures are not comparable. Though hysterectomy is far too common and is destructive, it doesn't have the same far-reaching health impacts as oophorectomy, and from our perspective, is not the same issue in terms of urgency. This is based on studies and data, and nothing else.
I also believe it's important to be up-front with Terms of Use when you are approaching giving medical advice.
Our primary goal is to address the life-threatening issues that surround removal of the ovaries, and morcellation of uterine sarcoma. 67, 260, 261, 264, 269
Women whose endocrine systems have been dysregulated know something is wrong with their bodies. 410,000 women a year have nowhere to turn for information and support when they start to fall apart. The surgery is so common and broadly-accepted that these women cannot find malpractice representation or guidance. The HERS Foundation has stepped in to fill a void created by medicine and unaddressed by a flawed legal system, and in some cases has provided value, but in other areas we differ on priorities.